Venous & Lymphatic Drainage of Lower Limb
VENOUS DRAINAGE OF LOWER LIMB
- All veins of lower limb are provided with valves to direct the venous blood towards the heart against gravity.
- Lower limb presents 3 distinguishable sets of veins..
SUPERFICIAL VEINS :-
- They lie in the superficial fascia.. consist of..
- Great / Long Saphenous Vein
- Small / Short Saphenous Vein
GREAT / LONG SAPHENOUS VEIN :-
- It is longest vein of the body.
- Contains 10 - 20 valves, having a fixed terminal valve at Sapheno-femoral junction.
- It begins at the medial end of dorsal venous arch of the foot where the medial marginal vein joins the arch.
Dorsal Venous Arch-
- It lies on the dorsum of foot against the bases of metatarsals with convexity distally.
- It receives 4 dorsal metatarsal veins, each of which is formed by the union of 2 dorsal digital veins.

Course -
It passes upwards lying 2.5cm in front of medial malleolus
Runs backwards & crosses the medial surface of tibia obliquely
![]()
Reaches behind the medial border of tibia near the knee and occupies the postero-medial aspect of knee joint
![]()
Ascends along the medial side of the thigh & passes through the spahenous opening
![]()
It ends by draining into the Femoral vein after piercing the cribriform fascia & femoral sheath at saphenous opening.
Structures Accompanying -
- In the Thigh- Medial femoral cutaneous nerve
- At the Knee- Saphenous artery (branch of Descending genicular artery)
- In the Leg & Foot- Saphenous nerve
Tributaries -
Just below the Knee-
- Posterior arch vein
- Anterior leg vein
- Communicating veins to small saphenous vein
In the Thigh-
- Antero-lateral vein
- Postero-medial vein (also called as Accessory saphenous vein)
Just before piercing the Cribriform fascia-
- Superficial epigastric vein (occasionally connected to lateral thoracic vein via Thoraco-epigastric vein)
- Superficial circumflex iliac vein
- Superficial external pudendal vein
After piercing the Cribriform fascia-
- Deep external pudendal vein
SMALL / SHORT SAPHENOUS VEIN :-
- It contains 7 - 13 valves.
- It begins at the lateral end of dorsal venous arch of the foot where the lateral marginal vein joins the arch.

Course -
It passes upwards lying below & behind the lateral malleolus
![]()
Ascends along the lateral margin of tendo-calcaneus
![]()
Runs along the mid line on the back of leg
Pierces the deep fascia between the two heads of Gastrocnemius & undergoes a sub-fascial course on the roof of popliteal fossa
![]()
It ends by draining in to the Popliteal vein at the middle of popliteal fossa
Variations in Termination -
- May drain into the great saphenous vein in the leg or upper part of thigh
- May bifurcate & drain into great saphenous vein & popliteal vein
Structures Accompanying -
- In the Leg- Sural nerve
- At the Popliteal fossa- Posterior femoral cutaneous nerve

DEEP VEINS :-
- They are surrounded by muscles & accompany the arteries.
- Eg:- Femoral vein, Popliteal vein, Tibial vein, Common peroneal vein.
- Below the knee most of the deep veins are arranged as Venae comitantes.
- Deep veins in the soleus muscle are arranged in the form of Venous sinuses.
Factors helping Venous Return -
In Upright position-
- Contraction of calf muscles (calf pump) (peripheral heart)
- Pulsations of arteries
- Valves in the veins
In Recumbent position-
- Contraction of heart & diaphragm during inspiration.
PERFORATING VEINS :-
- They pierce the deep fascia & communicate the superficial veins with deep veins.
- They are valved at each end & permit only the unidirectional blood flow from superficial to deep veins.
- There are Direct & Indirect perforators.
- Great & Small saphenous veins are considered as large sized direct perforators.
- Direct perforators are constant in number with fixed positions.
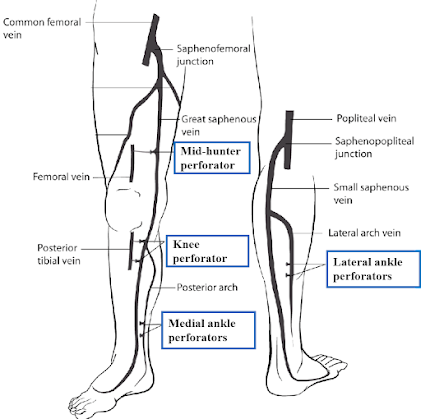
Positions of Direct Perforators -
- Mid-hunter perforator- Connects the great saphenous vein with femoral vein in the adductor canal.
- Knee perforator- Connects the great saphenous vein with posterior tibial vein below the knee.
- Medial ankle perforators- Usually 3 in number, connect the posterior arch vein with posterior tibial vein on the medial side of ankle.
- Lateral ankle perforators- connects the small saphenous vein with peroneal vein.
APPLIED ASPECTS :-
Varicose Veins -
Definition- Abnormally dilated & tortuous superficial veins.
Cause- Incompetence of venous valves, resulting in passage of high pressure blood from deep to superficial veins.
Tourniquet test-
- It is done to recognize the sites of incompetent valves.
- On a lying down position patient’s affected lower limb is elevated to empty the varicose veins.
- A rubber tube (tourniquet) is tied at the thigh & patient is allowed to stand with a gentle exercise.
- If the varicose veins fill within 30 sec, valves of perforators are incompetent.
- When the tourniquet is removed, if the varicose veins fill at once from above, sapheno-femoral valve is incompetent.
Treatment-
- Stripping operation for incompetent perforator valves- Great saphenous vein is avulsed by turning inside out after disconnecting it at its termination & at ankle or knee.
- Trendelenburg’s operation for incompetent sapheno-femoral valve- Great saphenous vein is detached at its termination & all its tributaries are ligated individually.
Deep Vein Thrombosis (DVT) -
Cause-
- Venous stasis- due to prolonged hospital stay or muscular inactivity, leading to..
- Thrombosis- thrombus formation at the site of venous stasis.
- Thrombophlebitis- inflammation may develop around the vein.
- Pulmonary Thromboembolism- thrombus may dislodge to form embolus which migrates to the lungs & obstructs the airways.
- Varicose Ulcer- may develop over the area of venous stasis.
Venesection / Phlebotomy -
- Surgical exposure of a vein for intravenous access when peripheral veins are collapsed in hypovolemic shock, infants & obese patients.
- Great saphenous vein is preferred because of its constant position in front of the medial malleolus.
- Care to be taken not to include saphenous nerve while ligating the vein.
Aortico-coronary by-pass Operation -
- In coronary artery by-pass grafting (CABG) operation, great saphenous vein is used for vascular grafting between the aorta & coronary artery distal to the obstruction.
- Because of the presence of valves the vein is grafted with its valves directed towards the coronary artery.

LYMPHATIC DRAINAGE
OF LOWER LIMB
- The lymph from lower limb is drained into inguinal lymph nodes, which are arranged into 2 groups - Superficial and deep.
SUPERFICIAL INGUINAL LYMPH NODES
- These are situated in the subcutaneous fat.
- Consist of upper & lower groups.

Upper Group :–
- Contains 5 – 6 nodes.
- Forms a chain below the inguinal ligament.
- It has lateral & medial nodes.
Lateral nodes -
- They receive afferent lymphatics from-
- Gluteal region & adjoining anterior abdominal wall below the umbilicus.
Medial nodes -
- They receive afferents lymphatics from-
- Subcutaneous tissue of anterior abdominal wall below the umbilicus.
- In male, penis including prepuce & scrotum.
- In female, vulva & vagina blow the hymen.
- Perineum & lower part of anal canal below the pectinate line.
- Cornuae of uterus.
Lower Group :–
- They are 4 or 5 in number.
- Accompany the lateral side of termination of great saphenous vein.
- They receive afferents from all superficial lymph vessels of lower limb except the vessels following small saphenous vein.
- They drain into external iliac nodes.
- Some traverse the femoral canal and intercepted by deep inguinal lymph nodes.
DEEP INGUINAL LYMPH NODES
- These vary from 1 – 2 in number.
- They lie on the medial side of femoral vein within the femoral canal (gland of Cloquet).

- Deep lymph vessels which accompany the femoral vessels
- Glans penis or glans clitoridis
- Superficial inguinal nodes
APPLIED
ANATOMY
- The upper group of superficial inguinal nodes may be enlarged due to spread of infection or malignant growth extending from lymphatic territory drained by these nodes.
- The lower group of superficial nodes are enlarged in diseases affecting the lower limb except the area drained by those lymph vessels following small saphenous vein.
- Syphilitic lesion of prepuce involves the medial members of upper group of
superficial nodes, whereas lesion of glans penis produces enlargement of deep
inguinal lymph nodes of Cloquet.